The always provocative Unspun asks how it is that Indonesia’s minister of health is shocked at the country’s HIV prevention failure. It’s a good question, most especially since before becoming minister just a few months ago, Nafsiah Mboi spent six years at the helm of the National AIDS Commission.
The failure was highlighted in the new UNAIDS report on the state of the epidemic. They estimate that the rate of new HIV infections in 2011 was more than 25% higher in Indonesia than it had been a decade earlier. That raises some questions for me: is an increase of more than 25% in HIV incidence (i.e. new infections) over 10 years really so shocking? Is the rate of new infections in Indonesia still increasing today? How do we know?
1) How shocking is an increase of 25%?
It rather depends on what the original rate was. The fact is, Indonesia had virtually no HIV epidemic in 2001, except in drug injectors and waria sex workers. In other words, the baseline rate of new infections in the largest risk populations (female and male sex workers, their regular clients, and gay men) was extremely low. If you go from four new cases a year to five new cases a year you increase by 25% but add only one new infection. If a high prevalence country goes from 10,000 incident cases to 11,000 cases, it has increased by just ten percent but added 1000 new cases. Which is the bigger prevention failure? I’m not saying that HIV prevention in Indonesia is a great success story; quite the reverse (see below). I’m just reminding people to beware of relative measures.
2) and 3) Is the rate of new infections in Indonesia still increasing now? How do we know?
The fact is, we don’t. Indonesia, which in the early 2000s built up quite a strong surveillance system, has seen that system break down rather badly, in part because of the effects of decentralisation and in-fighting between government departments which means that people who should be running the system are busy squabbling over project funding, and in part because of the small-mindedness of some of the donor-funded NGOs, who cared more about measuring their own little efforts and sucking up to their own pet partners in government than about supporting strong and transparent national systems. We can’t measure new infections directly, so incidence estimates are based on models that use information about overall infection rates (prevalence) from several years for several different population groups, together with information on risk behaviour, in some case. I’m frankly surprised that UNAIDS even published an incidence estimate for Indonesia, given the shockingly poor quality of the data available in the last 5 years. I note that the shied away from giving estimates for many of the other large countries with similarly diverse epidemics and patchy data: Brazil, China and Russia.
That HIV prevention failed in Indonesia is indisputable. The failure was totally unnecessary, but sadly inevitable given the choices the country and its “development partners” made. When infection rates were still low we measured very high levels of risk behaviour in key groups. We did very little about it, and what we did was more often driven by institutional needs and development fashion than by the needs of the people at risk. We kept measuring risk and infection and saw that risk was not falling and infection was rising. We spent lots of time and energy getting more money, then threw the money at the same failed approaches (including, in the most iniquitous example, treating people’s STIs with drugs we knew didn’t work because the Ministry of Health, the WHO, the drug companies and their various cronies couldn’t get their shit together to change the outdated national guidelines on treatment).
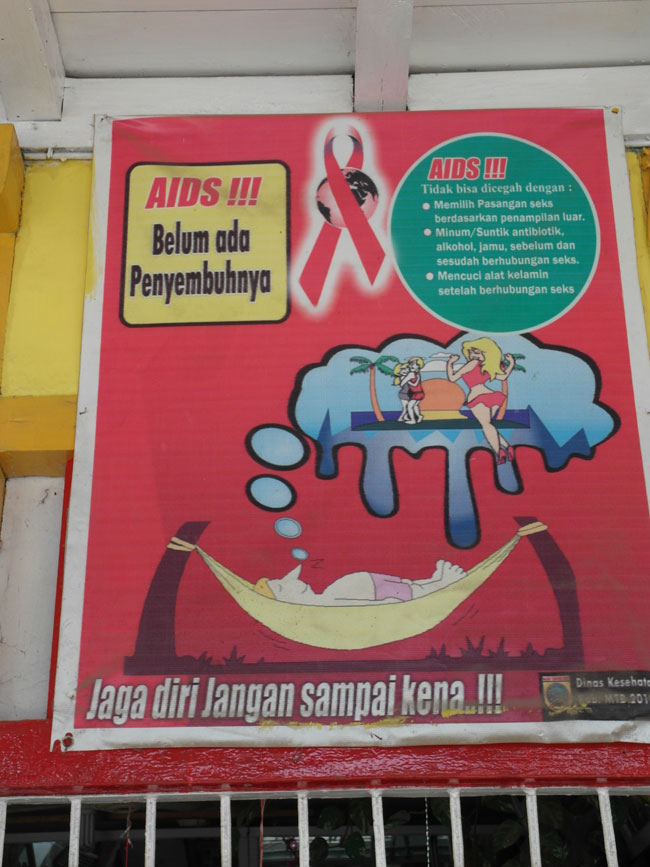
If what data we have are to be even remotely believed, there does appear to have been some success reducing new infection rates among drug injectors. But by 2009, three years into Nafsiah Mboi’s tenure as head of the KPA, Indonesia had sucked 60 million dollars into its HIV coffers, for that year alone. How much of that was spent on HIV prevention for gay men, a sizeable group in whom infection rates had rocketed from under 3% in Jakarta when I did the first study in 2002 to over 8% in 2007? A princely US$ 23,000. It’s not at all shocking that HIV prevention doesn’t work if you are simply not doing it. Or if you are doing the kind of thing Indonesia is mostly doing, pictured above. The poster reads: “Don’t ruin your life for just a moment’s pleasure. HIV/AIDS. You can get it, you can prevent it.” Does it tell you HOW you can get it, HOW you can prevent it? No. And there are even worse examples out there.
Here’s something that I found shocking: UNAIDS chief Michel Sidebe was in Jakarta just a couple of months ago. What did he talk about? Not the gay men, junkies, waria, rent boys and clients of hookers that make up four fifths of the Indonesian epidemic (the majority of other cases being in female sex wokers). Or at least not according to newspaper reports of his visit. No, he talked about the importance of protecting innocent women and babies through sexual education for young people, most of whom are at practically zero risk. (Reminder, you can’t get HIV by having sex, even unprotected sex. You can only get HIV by having unprotected sex with an infected person. As long as they stay away from the trade, most young heterosexuals in Indonesia can have as much sex as they like without risk of HIV infection.)
The highest UN official for HIV comes to Indonesia and stresses the importance of prevention for people who are not at risk, and Ibu Naf wonders why infections continue to rise in the groups that are at risk. Please deh! Someone should write a book about this.
Oh wait, I already did….